

We are in the early stages of major changes to the American health care delivery and payment systems spurred by the Affordable Care Act. This is a historic opportunity to move beyond simply providing acute episodic health treatment and instead create a comprehensive, efficient health system that makes the whole population healthier, Jim Hester, PhD, and PHI president and CEO Mary A. Pittman, DrPH, said in a web forum conversation.
Many health care providers and payers are currently rushing to experiment with reforms like patient-centered medical homes, bundled payments and accountable care organizations. These reforms mark important progress from Healthcare 1.0, which focuses on acute, episodic medical treatment to Healthcare 2.0, which emphasizes accountable provider networks, patient-centered care and a focus on prevention and care management. [This three-stage evolution of the health delivery system was developed by Neal Halfon et al in “Applying a 3.0 Transformation Framework To Guide Large-Scale Health System Reform” in Health Affairs].
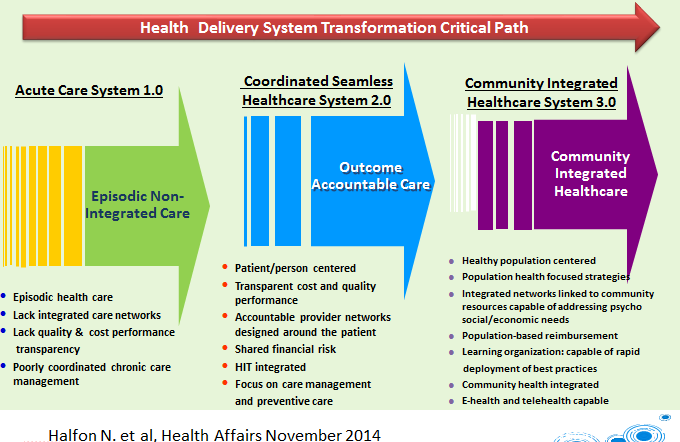
But Hester argued that the next frontier for innovation is in achieving Healthcare 3.0, which relies on new community-based population health models for improving health care quality and reducing costs that also integrate social and economic factors that drive much of health. So far there are only “partial models,” and few are ready to be taken to scale, said Hester, former acting director of the Population Health Models Group at the Center for Medicare and Medicaid Innovation. He is also a PHI board member.
“We’re still in a period of learning and experimentation” to understand how to build a financially sustainable community health system that incorporates population health, Hester said.
Looking for the Right Payment Model
And there is a risk that as health care payment reforms evolve they won’t incorporate meaningful population health components, he said.
Central to financially sustaining a community population health system will be a “balanced portfolio.” This would include financing for clinical services, ideally in the form of global budgeting. But it would also include investments to address “upstream” determinants of health, such as bike trails, YMCA diabetes prevention programs, expanded early childhood education to reduce adverse childhood events, and neighborhood grocery stores to increase access to healthy food. These investments need to match the specific health needs of each community.
Hester outlined an array of public and private financing mechanisms to support the portfolio. These included nonprofit hospitals’ community benefit funds, community development financial institutions, social impact bonds, foundation investments, prevention/wellness trusts, Medicaid waivers, Community Development Block Grants and Sustainable Communities Grants for transportation. A balanced portfolio would match the right intervention with the right financing mechanism and also include a mix of short-, mid- and long-term investments with varying degrees of risk.
The portfolio would be overseen by the “community health integrator,” an organization that would serve as the linchpin to the community population health system. The organization would be accountable for the health of the entire population within its geographic area, including reducing health disparities. The integrator would draw together health care, public health and community services to address the medical and nonmedical factors affecting health.
Pittman pointed out that some mainstream financial institutions are starting to develop mechanisms for investing in community health. But she also asked Hester what it will take to satisfy community skeptics that upstream improvements like bike trails will improve health. How can more investors be persuaded to “take the leap” to risk their capital on expanding community resources that impact health?
What’s needed, Hester said, is to draw on evidence of what works in the skeptics’ own communities.
Hester cited many examples of initiatives developing working models, including AHEAD (Alignment for Health Equity and Development), a partnership of PHI and The Reinvestment Fund; the Atlanta Regional Community Health Initiative; Live Well in San Diego County; and the Vermont State Innovation Model grant program. AHEAD is working to make community investments in health smarter and more focused in vulnerable places.
Pittman pointed out that PHI’s Center for Health Leadership and Practice also works to create multisectoral collaborations to improve population health, and PHI’s Build Healthy Places Network highlights strategies that bring together community development and health.
The Role of Public Health
Public health can help accelerate the transition to community population health systems, but some public health organizations will have to adapt to different roles in this new landscape. They might not always be the leader but instead act as a participant, a health strategy partner or the chief collaborator, Hester said.
“Public health has a major role, has an important role,” Hester said. “The way it plays that role … will vary from setting to setting because things evolve in very different ways.”
Act Quickly
Hester emphasized that the current period of health care system reform offers a “window of opportunity” of five to seven years to advance population health models. If the window closes, it may not open again for decades. He emphasized the need to pilot more community population health systems now and rapidly disseminate evidence of what works. New measures and analytic models are needed to measure meaningful and timely health, quality and cost outcomes at a population level across a spectrum of time horizons.
While he acknowledged the substantial work, and gaps, that remain, he and Pittman ended on a hopeful note. In more than 40 years of working in this field, “I have never been more hopeful that we can really move the needle and improve population health in this country,” he concluded.



You change the world. We do the rest. Explore fiscal sponsorship at PHI.
Together, we can accelerate our response to public health’s most critical issues.
Begin your career at the Public Health Institute.

Communities across the U.S. and around the world are grappling with dangerous wildfires and extreme heat. These threats disrupt and uproot communities and pose serious risks to environmental and community health—from rising temperatures, unhealthy air pollutants, water contamination and more. Find PHI tools, resources and examples to help communities take action and promote climate safety, equity and resiliency.