

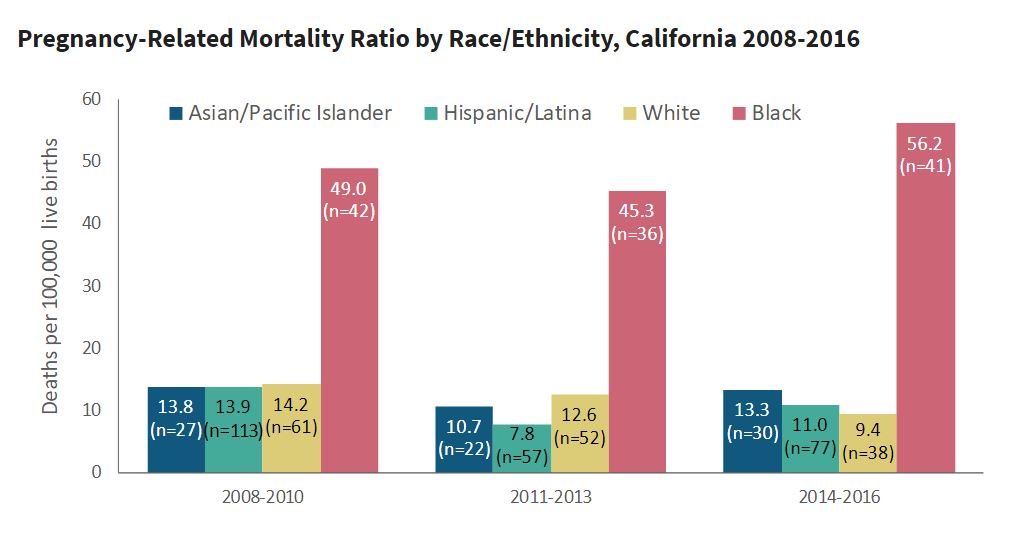
Released in September 2021, a California Pregnancy Mortality Surveillance System (CA-PMSS) report finds that California’s rate of pregnancy-related deaths has remained low compared with the U.S. rate and has been largely stable from 2008 to 2016. However, racial/ethnic disparities in pregnancy-related mortality ratios appear to be worsening, particularly among Black women. Black women were overrepresented among pregnancy-related deaths from all causes, especially deaths that occurred in pregnancy prior to birth or after delivery hospitalization.
While California has made progress to reduce maternal mortality through investment in maternal health programs, strong leadership and engagement of the maternity care community and targeted hospital quality improvement, more needs to be done to narrow racial/ethnic disparities.
See the reportThe California Pregnancy Mortality Surveillance System (CA-PMSS) is a statewide surveillance of deaths among Californians who were pregnant within the prior year. Funded by the federal Title V Maternal and Child Health Block Grant, the Maternal, Child and Adolescent Health (MCAH) Division of the California Department of Public Health (CDPH) initiated CA-PMSS and relies on a collaboration with three key partners: The Public Health Institute, Stanford University’s California Maternal Quality Care Collaborative, and a volunteer review committee of experts.
Pregnancy-related mortality was examined within the context of social determinants of health by incorporating the California Healthy Places Index, a validated measure of community well-being created by PHI's Public Health Alliance of Southern California. The HPI provides overall scores and more detailed data on specific policy action areas that shape health, like housing, transportation, education and more. California is among the first in the nation to include a validated measure of community conditions in the analysis of pregnancy-related mortality.
Originally published by The California Pregnancy Mortality Surveillance System
You change the world. We do the rest. Explore fiscal sponsorship at PHI.
Together, we can accelerate our response to public health’s most critical issues.
Begin your career at the Public Health Institute.

